
Nepal is in festive mood of Diwali (the festival of lights) and so is my family. This is a time for my family to gather, eat and enjoy. Cousins and relatives are gathered for the feast. They just called me downstairs to participate.
I just arrived from Gorkha which is a 5 hours
journey west from Kathmandu. Gorkha is the place where i am based to
support the rehabilitation of injured earthquake survivors through an
organization called International Medical Corps. As i arrived home, freshen up, had dinner but my mind was not letting me to go down stairs with my cousins to enjoy Diwali. So, i am aiming something new and different. Right
now, its 8 PM and I set my mind to do this write up about a woman with whom I met
in a health camp. Among the stories of various women with prolapse uterus, the story of Maya Gurung (name changed) was heart wrenching . Her
story shows how isolated and deprived the Nepalese Women are. She had a first degree
prolapse at the age of 20 and had been living with it till now. Her story says
how responsive our health and social system is? I believe her case represent
many Nepalese women living in various districts and villages of Nepal.
I was born and brought up in
Newari family which is one of the native inhabitants of Kathmandu, the capital
city of Nepal. During my childhood , i never felt how life in other districts of
Nepal would be like. Within one year, i got a chance to visit and stay in many remote corners
of Gorkha which is also an epicenter of Nepal earthquake 2015. I am proud to deliver
the rehabilitation services, being based in district level health system. Also one of the
greatest achievements for me was to gain an opportunity to understand the people,
their barriers and living situation.
The day before, was one of the
most memorable moments of my life as I was able to participate in the health
camp to deliver health service for women living with prolapse uterus in
remote villages of Gorkha. Within my organization, I played the pivotal role to
link rehabilitation services with sexual and reproductive health.
Thanks to my Organization for acknowledging the concept and
supporting me on full swing. I was also able to explain the importance of
preventive and rehabilitative role of physiotherapist to prevent and manage the
pelvic organ prolapse with concern official of ministry of health. For me,
it took almost a year time to formalize the process within my organization. The
day before was the first day I was involved as a team member of integrated camp
organized by District Public Health Office (Health tier in a district) for the
Women living with prolapse uterus and fistula. My job was to work in tandem
with doctors and nurses to deliver the comprehensive health services that also
included rehabilitation.
There are specific rehabilitation
protocols for the prevention and rehabilitation for prolapse uterus and fistula.
Many health workers are aware of Kegel exercise and thanks to previous training
programs to these health workers. The concept of exercises are always emerging
and changing as per new researches and so does apply for Kegel. On top of all, without the correct
demonstration and confirmation of perineum contraction, Kegel’s are most often
wrong and that gives opposite effect. Also programming the Kegel exercise
technique on daily activities like lifting the load is very important to
prevent the stress on pelvic floor.
Importantly, there are specific doses and implications for strength and endurance
for pelvic floor muscle that needs to factored in while designing the Kegels.
My experience says that for Nepalese women, intervention focused at minimizing
the risk of pelvic floor stress by teaching the safe way of performing
household chores is the most important preventive method.
Let’s come to Maya Gurung a
50 year old's story that made me to pause my Diwali celebration and made my mind
to do this write up at first. She had suffered from first degree uterus
prolapse during her first post-partum phase, 30 years back when she had
delivered her first son.
Immediately after delivery, she
had to carry heavy water pots and heavy wood and walk for an hour which
resulted in first degree uterus prolapse. She thought that’s a minor problem and
did not feel like seeking the service from health facility which is 7 hours
walking distance from her village. For her, priority were household activities rather
than seeking the treatment. Neither her husband nor family insisted her to
visit the health facility. This made the situation worse and aggravated to
third degree prolapse. Now she has complications like incontinence and abnormal
vaginal discharge which is degrading her health and self-esteem.
Now Maya says “I have difficulty
on defecation, feels like I am dying with the pain “ Her day starts from 2 am
in the morning to carry cattle fodder and carry water pots from a mile. It’s sad that she has compulsion to continue
her activities of daily living with difficulties. She felt that she is not
getting cured and won’t live longer. This feeling have made her more depressed and stressed.
With her eyes full of tears says “I am worried about my youngest daughter who
is studying in grade 7th as she is the most precious part of my
life”. I was surprised to know that her husband is a drunkard who rather than
lending helping hands, snatches her money for gambling. She has a small farm
and this has been her source of income to run a family but her ideas and
thoughts are not taken for family decision making. Her degrading health situation
has left her low esteemed that’s why she does not prefer to participate in
community functions and decision making events.
Let’s assess Maya using the
International classification of functioning (ICF) model
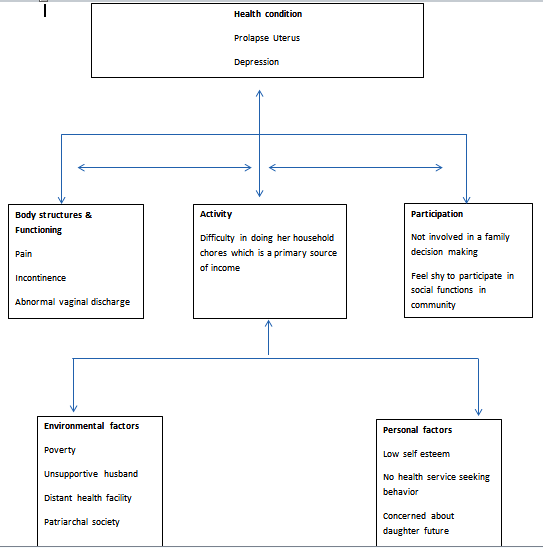
The main barriers for her was poor health seeking behavior which is linked to her and family illiteracy and
poverty level. Another one is distant health facilities that also further contributed to her
non health seeking behavior. The third one is our patriarchal culture in which
women are confined within the household chores which are stressful. In a course
of time, these three factors contributed for degrading health, low activity
level and participatory restriction in Maya’s life.
Maya’s story clearly depicts that
uterine prolapse is not only a health problem but it is entangled with
many issues like education, empowerment and economy of family. Therefore, a mutisectorial
, inter/intra departmental and inter/intra ministerial approach is a must.
This was the health camp where I participated, soon Maya will undergo hysterectomy and she will be cured.
But her other barriers will still remain the same that may further bring
complications like urinary incontinence and vault prolapse. Her husband is
still not supportive, her poverty line is still the same and she still has compulsion
to do heavy household works. There are many Mayas in Nepal who are living below poverty line. Isn’t it the time to think? Isn't it the time to
utilize the long experience(available data and lesson learn) to design the sustainable solutions?
Being a physiotherapist, I feel honored
to meet Maya and understand the situations of women living with prolapse in
Nepal. I know that my contributions to bring Maya to good living situation
through my physical therapy intervention are just like a drop in Ocean. Despite of all these, i am
hopeful that i was able to contribute at least a new and very important drop in the ocean, the
thing that has never started before(
Rehabilitation component added to prolapse uterus management). This has definitely ensured a multidisciplinary approach of care. Maya, now knows how to do her activities with minimal stress on her pelvic floor and what relieving position/exercises to do if she experiences a sudden difficulty. Again she will require physical therapy intervention after surgery to prevent the complications like incontinence and vaginal vault prolapse.
Nepal has 1800 physiotherapists
but not more than 20 quotas are allocated by ministry of health in the health
system. Ministry of health has Nepal health sector strategy, national prolapse
uterus management guideline, health worker training manual for fistula and prolapse uterus management,
national childhood disability management strategy, birth defect surveillance
and control plan as the guiding documents that strongly support to have physiotherapist
in a health system. Also there are sufficient human resources in the country
now. At this favorable situation (where human resources are available to fulfill
the service demands), Nepal should not make any delays to deploy
physiotherapists into the health system.