Early
childhood development (ECD) framework of UNICEF states that from conception
through birth to eight years of age is crucial timeline for child development.
Here, development reflects not only physical growth but also the cognitive,
emotional and interactions with each other(1). The main
focus of ECD is to ensure that a child is healthy from all the aspects which mean
promoting optimal functioning and participation. Having said this, ECD is not
only limited to health as we know that health is largely influnced by its
determinants. For children, some of the
important determinants of health are mother’s health, family support,
educational opportunities and access to services. There are certain services that children would
need at the course of growth and development out of which nutrition as well as
immunization are the most important ones. These two types of health care are
directly related to preventing the unwanted deaths and promoting the health of
children for a long run. For young children,
every day environmental scenario is something new. Hence, they might need
facilitations to overcome such new challenges. For example, going to toilet for
the first time might need assistance from family members. Therefore, family care and stimulation provides
nurturing environment to the children which are also essential components of
ECD. The real world is an interaction with not only family members but also to
peers. Hence, facilitation of peer activities in the form of play is another
important area to stimulate the components (including emotional and cognitive)
of child development. Schooling is an important means of early child development
that provides further cognitive, emotional and physical stimulation to nurture
the growth and development.
Now
let’s understand the scenario of children with disability from ECD point of
view. The scenario might look complex because the child is disabled now which
means he or she may not show the same level of activities compare to the child
of same age. So, how does the nutrition and immunization service work for such
child? What are added responsibilities of family members? Very importantly, how
do we ensure the peer interaction, play and educational support which are also
the important components of ECD? Before probing these questions it is quite
vital to detect the impairments. The important and perhaps the first step to
answer is, how do we confirm the impairment? What are the roles of health
workers, family and teachers for the detection?
From
the child protection act (1992), National Planning and Plan of Action on
Disability in Nepal, (2007), UNCRPD, to Incheon strategy (2012), there had been
mentioning of ECD and its components. Also, these commitments are gradually being
converted into the budgeted actions of Ministries as well as agencies, for
which we have to acknowledge the advocacy made by right holders and service
providers in childhood disability sector. According to the living condition
study, the commonest cause for disability in Nepal is congenital/by birth which
means more people start acquiring disability from the birth. The same study
reported that 43.4% of disability is acquired by birth to the fifth years of
life(2). Actually,
real prevalence in children is more than what was reported because these
estimations were made based on Washington group questionnaire which is not
sensitive enough to detect the problems on developmental and cognitive
functioning. (As explained below)
In
any settings the confirmation of disability is the starting point to address
the ECD need of children with disability. In fact, after the endorsement of
international classification of functioning (ICF) by WHO, the school of thought
to define disability has been drastically changed. But having said this, it is also important to evaluate
how far the signatory countries are progressing on shifting the medical model
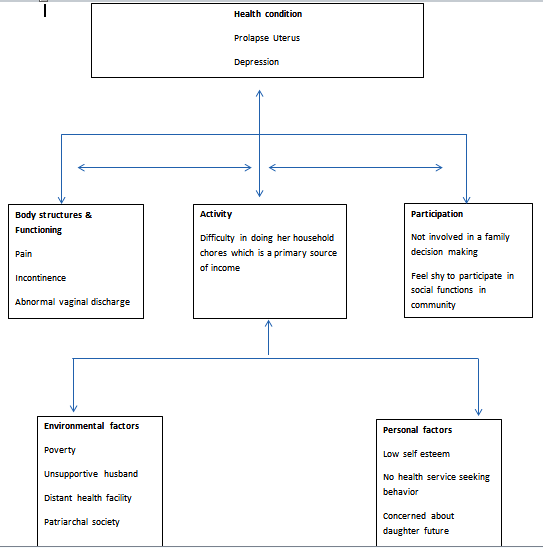
of disability intervention to the biopsychosocial model as defined by ICF(3). According
to ICF, disability is the state of functional limitation or participatory restriction
(because of functional limitation) due to the negative interaction between
medical conditions, personal factors (motivations, confidence, willpower of the
person etc.) and environmental factors. Here, environmental factor means not
only the physical environment but also other contextual elements like support
from family members, access to varieties of services, leadership & governance
of the sector etc.
I
would like to share a simple example which is based on my experience on working
with children with disability. There were two children living with bilateral
clubfoot, belonging to one of the hilly districts of Nepal who were detected by
“Early Detection” trained health workers. Both the family members could not afford
the transportation, accommodation and fooding expenses to go to nearest rehabilitation
center (100 KM away) where service charge for families belonging to poor
economic back ground is usually waived. Then the decision was made to cover out of
pocket expenditure of both families. Surprisingly, one family did not take the
child for treatment while the next did. Very recently, I had a follow up visit
to the same place and could gain a visible impact on a child who has gone through
the treatment while a child was walking properly and family members were quite
happy to the progress made by a child. The foot of a child who did not undergo treatment
was deteriorating. It was also discovered that father was uncooperative and drunkard.
Although mother wanted her child to get timely treatment she was forced to get
bounded to her household chores and could not travel alone. Neither her husband
accompanied her to treatment center nor was she confident enough to travel
alone. From this example, it can be well understood that how important is the family
support which is one of the contextual elements. Even though the medical care
was guaranteed, the child did not have access to it because of contextual
barriers. Thus, only medical focused intervention may not always address the disability
issue that is why we need to visualize disability from wider lens which is the
combination of medical, psychological and social factors.
Also, my experience says that
structural impairment (physical) disability are quite visible which might be
detected at the health facility or school level once after providing short term
training or orientation . But the detection of disability affecting emotional
and cognitive components of ECD might need more training and focus as these
types of impairment are not directly visible in a snapshot. Family members should be central to the
disability detection as they are in the best position to explain what they have
observed in child. Detection or medical diagnosis may not fully contribute to
address the ECD need of child. To facilitate
the early childhood development of children with disability, we need to know
what child can do and what not as per his/her age threshold. That’s why we need
to assess disability in terms of functioning across the domains of physical,
emotional and cognitive areas.
As
explained above, ECD primarily constitute growth and development in physical,
emotional and cognitive aspects which means that each of these elements needs
to be assessed while we confirm the disability on children. In many stances
disability might appear as a mix of these elements.
Let’s
talk about the very recent advancement on the data collection of the children
with disability (2-17 years). UNICEF in
collaboration with the Washington group on disability statistics has
developed the module on child functioning for identifying children with
disability on surveys. This module is precursor of previous tool like Ten Question Screening Instrument and previous short sets of Washington Group on
Disability (4)(5) (6). The new
child functioning module is more sensitive to previous tools as it is able to
detect the developmental and behavioral components of the disability in
comparison to previous tool. It means that now we have the tool in place which
can detect more complex and invisible type of childhood disabilities. The new
child functioning module might not include 0-2 years as same age group is not sufficient to confirm the functional limitation. In Nepal,
it is widely claimed that the present 1.94% prevalence of disability reported
by 2011 census is far more than the actual prevalence of disability as simple census data collection process might
had missed to detect disability that are
not visible. Hence, THE NEWLY DEVELOPED MODEL BY UNICEF gives an opportunity to ensure the inclusive data collection (covering all the aspects of ECD). For sure, partnership among right holders association, UN agencies, service providers and decision makers should be the key strategy to have such survey implemented in Nepal.
I will be
writing my next blog on the link between early detection and inclusive
education from the perspective of ECD. Please stay tuned.
I
welcome your feedback and suggestions.
(This is my
personal blog where I present my personal write ups hence it reflects my view only)
References
1. Early Childhood Development
[Internet]. [cited 2018 Aug 14]. Available from:
https://www.unicef.org/dprk/ecd.pdf
2. Eide AH. Living conditions among
people with disability in Nepal. SINTEF Rapp. 2016;
3. WHO (World Health Organization). World
report on disability 2011. Am J Phys Med Rehabil Assoc Acad Physiatr
[Internet]. 2011;91:549. Available from:
http://www.ncbi.nlm.nih.gov/pubmed/22726850
4. Cappa C, Mont D, Loeb M, Misunas C,
Madans J, Comic T, et al. The development and testing of a module on child
functioning for identifying children with disabilities on surveys. III: Field
testing. Disabil Health J. 2018;
5. Massey M. The development and testing
of a module on child functioning for identifying children with disabilities on
surveys. II: Question development and pretesting. Disabil Health J. 2018;
6. Loeb M, Mont D, Cappa C, De Palma E, Madans J, Crialesi R. The development and testing of a module on child functioning for identifying children with disabilities on surveys. I: Background. Disabil Health J. 2018;
6. Loeb M, Mont D, Cappa C, De Palma E, Madans J, Crialesi R. The development and testing of a module on child functioning for identifying children with disabilities on surveys. I: Background. Disabil Health J. 2018;